
Read the PDF version of the article
A forgotten disease: With the help of a Houston billionaire, an ex-president and an army of volunteers, millions of Africans will be spared from river blindness
By CLAUDIA FELDMAN
Houston Chronicle
ADDIS ABABA, ETHIOPIA - Down by the Wanja River, naked boys swim through the swirling currents with whoops of joy.
Women scrub clothes at the water's edge, and farmers, men and women, chop weeds for hours on end.
Only tiny black flies disturb the peace. They bite, and some days the sounds of people slapping at insects can be heard throughout the lush river valley.
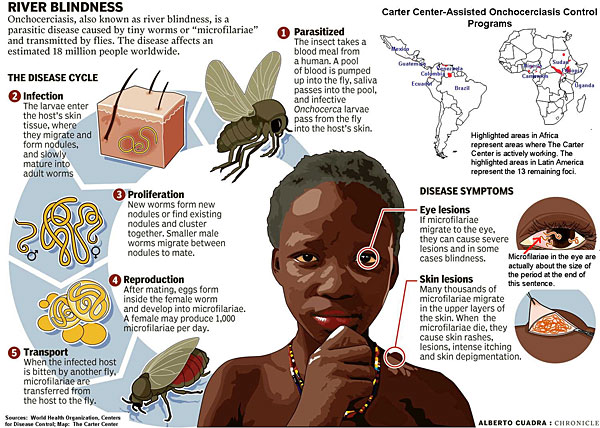
The infected flies spread the tropical scourge onchocerciasis.
And fear.
The disease, often called river blindness, starts with itching. It can get so severe that fingernails don't satisfy, and sufferers scrape off layers of skin with sticks and stones.
The frantic urge to scratch is caused by parasites, tiny worms implanted under the skin by infected flies.
As the worms mature, the females grow up to 18 inches long. When they spawn, they produce millions of offspring, known as microfilariae. Some of them will migrate to the eyes.
Roughly 123 million people live in areas where the disease is endemic, which means they're at risk. Eighteen million people in 37 countries, most in Africa, wrestle with the itching, the mottled, leathery skin, the physical exhaustion, the social rejection that are part and parcel of the disease. About 500,000 suffer from low vision, and 270,000 have gone blind.
There is a solution - it's a couple of free tablets, taken once a year.
The medicine is ivermectin, also known as Mectizan, and it relieves symptoms and preserves sight. From the Western view, that's not hard. River blindness should be relatively easy to control.
Onchocerciasis experts say tremendous strides have been made in the fight against the disease and that the battle eventually will be won. Public health organizations target it for eradication in the Americas and for control throughout Africa in the next 10 years.
"It's a wonderful success story," says Dr. Frank Richards, technical director of the river blindness program for the Carter Center, a nonprofit humanitarian organization based in Atlanta.
He admits, however, that he prefers to describe ongoing efforts to combat the disease as a glass half full.
At present, 52 million treatments of Mectizan are administered every year. But, discounting the pregnant women and children under 5 who can't take the drug, 50 million people still need to be treated. Others are treated too late.
Ethiopian Negash Bitena, 65, falls into that last category. He lives at the end of a long, muddy trail in the village of Tassano with two sons and a daughter.
He has river blindness. Before his wife died, she also suffered from the disease, and their 25-year-old daughter is afflicted as well.
In a deep and gravelly voice, he explains that river blindness dims his vision, drives him crazy with itching and saps his strength.
"I am miserable, as you can see," he says.
Inside his stick house, a cow weighing close to 1,000 pounds takes up half the space.
Bitena explains that the cow is all they have; they can't afford to lose it by keeping it outside.
Amarech, Bitena's daughter, listens quietly.
She was in first grade when her itching started.
"My mom was taking care of me," Amarech says. "Unfortunately, she died."
Over the years, her skin has hardened and the color has darkened. Her vision is blurred.
"When I think about the future, I feel completely hopeless," she says. "The Mectizan can't give me a dramatic improvement. My vision can't be restored. My skin is destroyed.
"I would have liked to be a doctor," she says wistfully. "Maybe a government employee."
Suddenly the problem that looks simple isn't simple at all. Instead, it's the story of Africa, dense and complicated.
In Africa, no problem stands alone. Money and muscle don't talk the way they do in the West, and the successes that stick have to be engineered from the bottom up, by insiders, not from the top down, by outsiders.
"Hey, everybody wants to argue that the glass is half empty in Africa," says Richards, objecting. "That's the usual thing."
Even he admits, however, that defeating river blindness sometimes seems like the tip of the hippopotamus' ear.
A long list of problems bedevils Africa - gut-wrenching poverty, political upheaval, poor leadership, minimal public health care - and the list goes on. Richards and Dr. Donald Hopkins, associate executive director of health programs at the Carter Center, are well aware.
Keep pushing forward, Hopkins says.
Diseases are conquered in Africa, and for that matter in the United States and other developed countries, one step at a time. He adds that the knowledge gained in the battle against onchocerciasis will help in wars against Africa's killing diseases - malaria, HIV/AIDS and tuberculosis.
"We're lighting a candle in the dark," Hopkins says. "In an imperfect world, on a troubled continent, it's very important to do this work. We can't allow ourselves to be paralyzed."
In the lab
In 1975, Dr. William Campbell realized that ivermectin, medicine being testing to deworm domestic animals, might help river blindness patients, too.
The "aha" moment came as Campbell was studying a parasitic worm that plagues horses, and he realized it bore a startling resemblance to Onchocerca volvulus, the river blindness parasite.
"It was just a simple connection," the 75-year-old retired Merck scientist says modestly. "I saw tremendous potential, but I thought it was too good to be true."
Still, he reported the news to his bosses.
"We could only permit ourselves a very subdued excitement," Campbell says. "We knew a million things could go wrong."
They were keenly aware of another promising river blindness drug that had gone south.
In the 1950s and '60s, other researchers worked with the drug, diethylcarbamazine, commonly known as DEC. It controlled parasites in animals and was considered briefly as a weapon in the onchocerciasis war.
But patients who took it experienced additional skin rashes and accelerated vision problems. Those on course to lose their vision in 10 years went blind in three weeks.
Another, far more successful attack was launched in the early '70s by the World Bank. Robert McNamara, then president of the organization, was traveling through West Africa when he saw scores of blind adults being led around their villages by children with sticks.
Deeply moved, the former secretary of defense announced the World Bank would fight the disease by spraying insecticide in the river valleys where the black flies bred.
"The campaign was highly effective; it did what it was supposed to do," Campbell says. "But it devolved. When it came time for the individual countries to take charge of the spraying, they couldn't handle it. They didn't have the expertise or the funds."
Meanwhile, Campbell and his team plugged away on ivermectin.
"We persisted," says Campbell. "Our drug turned out better than we could have hoped."
Mectizan has proved to be safe and effective in killing the microfilariae, the baby worms that cause low vision and blindness.
Taken annually, the tablets relieve the intense itching and eliminate other parasites, though it does not reverse damage already done.
Mectizan's main limitation is that it does not kill the adult worms. Patients must wait for them to die naturally, a process that can take 10 to 15 years.
Richards, with the Carter Center, still remembers the reaction to the drug and Merck's 1987 pledge to donate it as long as needed. The gift, to date, is worth $1.5 billion.
"People said, 'Nice, but this isn't what we want. Go back to the drawing board.' "
Richards says the naysayers missed the point. He compares Mectizan to flu shots. It would be nice if they offered lifelong immunity, but a year's protection is still invaluable.
"Take Mectizan," he says. "You won't go blind, and you won't itch."
A benefactor emerges
On Jan. 23, 1990, billionaire philanthropist and computer software guru John Moores lingered over his morning paper. The Houston Chronicle story that grabbed his attention featured University of Houston optometrist Bill Baldwin. And river blindness.
Like McNamara, Baldwin had been to Africa, and he was haunted by the vision of blind men and women guided by children. Baldwin knew how difficult it was to deliver Mectizan to the people who needed it, but that's what he wanted to do. He had a plan.
Moores, who has changed the face of the UH campus with the size and breadth of his gifts, invited Baldwin to what turned out to be a $4 million lunch.
Together they started the River Blindness Foundation, dedicated to putting pills in the mouths of millions and turning the tide of a disease out of control.
Ultimately, the Texans knew African leaders had to be sold on the efficacy and safety of the drug. Those leaders had to educate the people below them, who had to educate the people below them. That would take time. African leaders also had to find volunteers in villages to help administer the pills.
The key was that they had to do it. Africans. Villagers weren't going to listen to strangers telling them what to do.
Moores says he knew that from the get-go. It's hard to win trust, he says. And it's hard to give money well.
"It's the law of perverse consequences, or the law of unintended consequences," he says. "The classic example is you find people hungry, give them food, and in the process destroy the local economy. It's hard to compete against free.
"At the same time, there's no downside to keeping people from going blind or putting them back to work. I like that model. And I haven't found a better use for money."
By the mid-'90s Moores had spent $25 million on the cause, earned the attention of former President Jimmy Carter and looked forward to merging the River Blindness Foundation with the Carter Center. One of its missions is to help forgotten people with forgotten diseases.
"For me, that was a godsend," Moores says. "Carter's shoulders are very broad, and he's able to go out and raise a lot of money."
Moores, who lives in San Diego now and owns the Padres baseball team, still has a home, business interests and friends here. He also spends increasing amounts of time in Atlanta. And he makes long treks to Africa. In mid-September, he gave interviews in a hotel lobby in Bahir Dar, Ethiopia. He and Carter had spent the morning viewing latrines built by villagers struggling to control another preventable blinding disease, trachoma.
During a long and hot program, Carter did the talking. Moores played with the village kids. He took pictures. That, joked the native Texan, was his job.
But Moores grew serious when he talked about his mission. "As Americans, we just write off Africa. As far as I can tell, every soul here is just as important as every soul north of the Rio Grande."
A firsthand look
Teshome Gebre, an Ethiopian whose brother lives in Houston, understands Americans well. He's attended public health conferences all over the United States. He earned his master's degree from the University of New Mexico. He speaks English almost perfectly.
But his heart is in Africa. He, his wife and their children live in Addis Ababa, and he oversees the Carter Center health programs in Ethiopia.
When Carter and Moores visit, he takes them to meet the poorest of the poor, the people suffering from diseases targeted by the center.
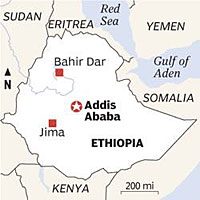
On a sunny day in September, he takes a small group from Addis to Jimma. That's six hours, past donkeys stumbling under loads of hay, past women with baskets on their heads, past men carrying jugs of water balanced on poles on their shoulders. The landscape is impossibly green. The air is warm and heavy. It has just rained, and in a matter of hours it will rain again.
Half an hour past Jimma, the smooth roads give way to potholes and gravel. Every few miles there are villages, each one poorer than the last.
Houses and businesses are made of sticks and mud. There's no running water, few signs of latrines and no electricity.
On the road, cows, goats and sheep bleat and bellow for the right of way amid trucks and SUVs. In the distance there is the occasional flash of monkeys perched in trees.
Banana trees, orange trees and coffee plants grow wild. In the background are purple mountains, fertile valleys and fast-running streams.
In these communities, river blindness is a common heartbreak, but only one of many.
At the Carter Center's request, river blindness patients from the villages of Afeta and Kenteri gather at Spartan government clinics.
In Afeta, Gebre greets the clinic staffs and checks their records. Almost 6,000 residents have received Mectizan in 2004 and 2005. That's good, but the scores of patients milling around the clinic paint a picture of despair.
Many have had river blindness for 10, 20 years. Problems - distribution, organization, leadership, money - kept them from getting the Mectizan until it was too late.
Gebre greets patients one by one and tries to speak their native tongues. That's difficult. Ethiopians live by a different calendar from Westerners, they keep time differently, and they honor 80 local languages.
Helping to translate is Nasir Abdo. He works for the government as program coordinator for onchocerciasis in Jimma. Together, they work the crowd.
Patients, all ages, are dressed in thin, patched clothes. If they have shoes, they don't fit. Those who are barefoot have blackened nails, calluses, feet like hooves.
Ethiopians are known for their big eyes, beautiful skin, fine features. But some of these patients are so thin their noses protrude, beaklike, and their cheeks are sunken. Their legs are broomsticks, rattling around under frayed pants.
The men show their shins so Gebre and Abdo can see their spots.
They have scratched so much they are permanently scarred. They call it leopard skin - mottled black and white.
Most patients talk so fast it's impossible to translate it all. But at the end of the bench on the clinic porch is Hadhameded Abafogi, silent. She's 40, a widow, destitute, blind.
Her son helps her, she says when she finally speaks to Gebre, who is translating. "I can't do anything for myself. Even to visit the toilet I need help."
She's had two doses of Mectizan, given after the worms had wrought their damage.
Her voice is low, dejected. "I used to be independent and go where I liked."
She thinks long and hard when asked if she has hope for the future. Finally she says, "I hope my eyes will be opened, and I can see the light."
The public health officials know that's not going to happen. They flinch.
Around the corner is Momina Abadura. She is 30, a wife, a mother of five, a farmer as Abafogi had been.
Abadura still has her sight, her energy. She looks barely scathed by the disease until she goes behind the clinic and raises her dress. The skin from her shoulders to her buttocks is rough and leathery, and she has multiple scars from scratching.
"My husband is sympathetic," she says, "but mostly I don't talk about it. I'm embarrassed, ashamed. People might point their fingers."
She's right. Villagers often treat river blindness sufferers as if they are contagious, contemptible.
Shaken, Gebre and Abdo climb back into SUVs - regular cars wouldn't make it on this treacherous road - and head for the clinic in Kenteri. Again there is a long line of onchocerciasis sufferers. One invites Gebre and Abdo to his home.
It's just across the road, a mud hut. Wole Hamza built a second structure just a few feet away, but it leaks.
Hamza, standing ramrod straight, introduces his wife, four children, one granddaughter. All seven sleep together, some just inches from the campfire.
His life used to be so much better, he says. "With oncho, I'm itching, I'm suffering, I'm emaciated. This disease robs me of my courage to work, to travel."
He has other problems, which he is happy to list. Most telling is the desperation in his cloudy eyes. He has to feed his family. The question is how.
Gebre, translating, won't repeat reporters' questions about food. The trip, for him, has become very personal. He feels protective.
"We must leave the people their dignity," he says.
The answer is obvious. There is no food except the oranges hanging on a nearby tree. They are not enough.
The next morning, there are two more home visits.
Ababora Abajobir, 70, is waiting for company. His hut is scrupulously clean. It used to be nicer, he says, back when he had a metal roof.
He sold it, he says, when he and his children had nothing to eat.
Now the roof is straw and plastic, and, of course, it leaks.
Again, onchocerciasis is just one agony in his life. Over the years he has lost five of his seven children to ill health. His wife is dead, too.
"She had a broken heart," he says.
Abajobir worked his coffee farm until his illness and age caught up with him.
"I'm poorer and poorer," he says. "Weaker and weaker."
These days Abajobir spends much of his time in bed.
"I wish I could tell you," he says to Gebre and Abdo, "something that makes me happy or joyful. My only hope is my grandchildren, that they can manage to succeed."
The last home on the tour belongs to the Bitenas, who share their dwelling with a cow.
Gebre looks ill himself when the sick daughter speaks of the future she might have had. He looks worse when she says she's never had a boyfriend and knows she never will.
"Every day," he says on the trip back to Jimma, "we don't know who or what we're losing."
In the evening, Gebre's mood is darker still. He is no longer speaking for the Carter Center, he says. He is speaking for himself.
Why do Africans suffer with problems beaten by developed countries decades, even centuries ago?
He asks the question, and he answers it.
"Because our economy goes from bad to worse. Because development resources are not utilized. Because there is poor management, poor government. We fight among ourselves instead of tackling our common problems."
Teaching good health
Hard to say if the glass is half empty or half full in an elementary and middle school in Afeta.
More than 60 children are crammed into a fourth-grade classroom made of mud. There are no windowpanes, no lights.
When asked if they've taken Mectizan, they raise their hands. They're excited. Yes!
They know about river blindness and trachoma and the importance of keeping themselves clean.
Yes!
What do they want to be when they grow up?
The brave ones raise their hands.
A doctor.
A driver.
A professor.
A self-possessed child in the corner says she wants to be president.
The teachers, the parents, the students are doing the best they can.
Back in his Addis Ababa office, Gebre has cheered up. He is proud of his country, he says. "We claim a history of 3,000 years. We were one of the first countries to accept Christianity. Most African countries were colonized by the West. We were not. For a short time we were occupied by the Italians, but we fought back fiercely, furiously. Our culture remained intact."
Gebre, married to a schoolteacher and the father of four, has worked in public health in Ethiopia for almost 30 years. He helped eradicate smallpox. He's trying to zap polio and neonatal tetanus. He hopes to work 10 more years, long enough to see the preventable blinding diseases trachoma and river blindness eliminated.
Gebre has many other hopes for his country, and it would be sweet if he could retire on a wave of success.
He smiles ruefully.
If he can't meet his career goals soon, he will have to do what the river blindness patients do - put his faith in his children. And their children.
Unbelievable that it is so difficult to battle a fly and a worm.
Used with permission. Copyright 2005 Houston Chronicle Publishing Company

Photos: Steve Campbell / ChronicleDAILY LIFE:Amarech Nagash, 25, cooks for her family in the village of Tassano, Ethiopia. She, her mother and father have all suffered from river blindness.

OUTWARD SIGNS:Tadese Teklie's leg bears the telltale signs of river blindness. He waits with other patients at a government clinic in Kenteri, Ethiopia.

LITTLE HOPE:Amarech Negash once hoped for a career and a family of her own. Now that she has river blindness, she has abandoned those plans.

INTENSE PAIN:Amin Hussain, who lives in Afeta, takes Mectizan to combat a troublesome symptom of river blindness -- intense itching.

FIGHTING BACK:Abebe Mekonen walks away from his family's latrine. Good hygiene helps control another preventable blinding disease, trachoma.

HUMANITARIAN EFFORT:John Moores, chairman of the board of trustees for The Carter Center in Atlanta, photographs a latrine in Mosebo. The latrines cost virtually nothing to construct but give dignity to residents and help in the fight against the preventable blinding disease, trachoma.

SILENT VICTIM:Wole Hanza, who has river blindness, sits in his hut in Kenteri. The disease has left him wasted, and he is struggling to feed his family.

FIELD OF DREAMS:Almushe Adugna and her husband, Asfa Bekele, weed teff fields while their daughter, 2-year-old Wobalem Asfa, rides on her mom's back. They live near Mosebo, which is trachoma country.

RICH TRADITION:Coffee is a huge crop in Ethiopia and a drink enjoyed by all. Tegei Fenta roasts these beans over an open fire as part of a traditional coffee ceremony.
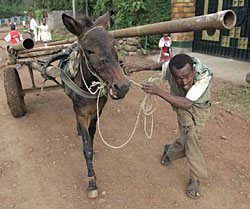
AT WORK:Agmasde Demala ducks as his load of pipes shifts. Animal powered carts are a common sight in Bahir Dar and throughout Ethiopia.

BLOSSOMING:In September, Ethiopia is ablaze with these yellow flowers that resemble candle sticks.

HELPING HAND:Hadhameded Abafogi, left, blinded by onchocerciasis, is led from a public health clinic in the Ethiopian village of Afeta by her 20-year-old son, Yassin Abafogi.

THE CURE:Nurse Roman Addisu, left, gives Mectizan tablets to Hussein Mohammed, 55, in the village of Kenteri. Since there are few reliable scales in rural Ethiopia, a volunteer worker measures Mohammed's height to determine his dosage.

WAITING GAME:Tadu Ababora, from left, Rahmatu Oli and Bultu Abagaro sit under a river blindness prevention poster at a Kenteri health clinic.

SPREADING THE MESSAGE:Sara Biya, from left, Derartu Biya and Semira Biya answer questions about onchocerciasis in a fourth grade classroom in Afeta.Those with their hands raised have had the drug, Mectizan.
RESOURCES

DISEASE CYCLE:
BLOG:
RIVER BLINDNESS BY THE NUMBERS:
Source: the World Health Organization
FAST FACTS ON ETHIOPIA:
Please sign up below for important news about the work of The Carter Center and special event invitations.
{kind=link}